Retake
R7) Scrotal pain and swelling
Review the Learning Outcomes, Hx, PE and Labs, and begin the module with your Provisional Diagnosis. Keep hitting "Next" to move through the module.
Learning Outcomes
- Articulate your relationship with the consulting diagnostic radiologists in the evaluation of a patient with testicular pain.
- Review the DDx considerations in testicular pain.
- Identify the spectrum of imaging findings in appropriate modalities for evaluating patients with testicular pain.
History
A 25-year-old male presents to his primary care physician after experiencing five days of worsening pain localized to the right side of his scrotum, accompanied by noticeable swelling and erythema. The patient reports a perceived increase in the size of his right testicle. He provides a sexual history indicative of high-risk behavior, specifically mentioning his practice of receptive anal intercourse with multiple partners.
Physical Exam
Vital Signs: BP 130/86 mmHg, HR 60 beats/min, RR 18 breaths/min, Temp 100.4°F, SpO2 98% on room air.
Genitourinary Exam: Pain is alleviated with elevation of the testis. The cremasteric reflex is intact. Both the epididymis and testis on the right side are tender on palpation. Comparatively, the right testis appears larger than the left and transillumination is positive.
Labs
None
Provisional Diagnosis
Select the Dx you believe is most appropriate
Epididymo-orchitis appears to be the most probable diagnosis. While testicular torsion was initially considered, this seems less likely due to the presence of a positive cremasteric reflex and relief of pain upon testicular elevation (Phren's sign).
Well done. You were correct
Potential Acuity
What is your assessment of the likely acuity for this patient?
Well done. You were correct
The patient's condition necessitates urgent evaluation and further diagnostic workup. It is critical to definitively rule out testicular torsion, as delay in diagnosing and treating this condition could potentially lead to testicular loss.
First Imaging Study
What is the first imaging study you will order?
Scrotal ultrasound is the best imaging modality to evaluate acute scrotal pain. In many cases epididymitis can be diagnosed clinically, but a scrotal ultrasound can rule out testicular torsion. Ultrasound is used to assess the structural and functional anatomy of the scrotum. Furthermore, color doppler is helpful in diagnosis; increased blow flow often represents infection and decreased blood flow often represents torsion. Additionally, ultrasound can help determine whether there is formation of a reactive hydrocele or abscess.
Well done. You were correct
Pertinent Imaging Observations
Click on the links below to view images from the study, and assess these key findings as best you can.
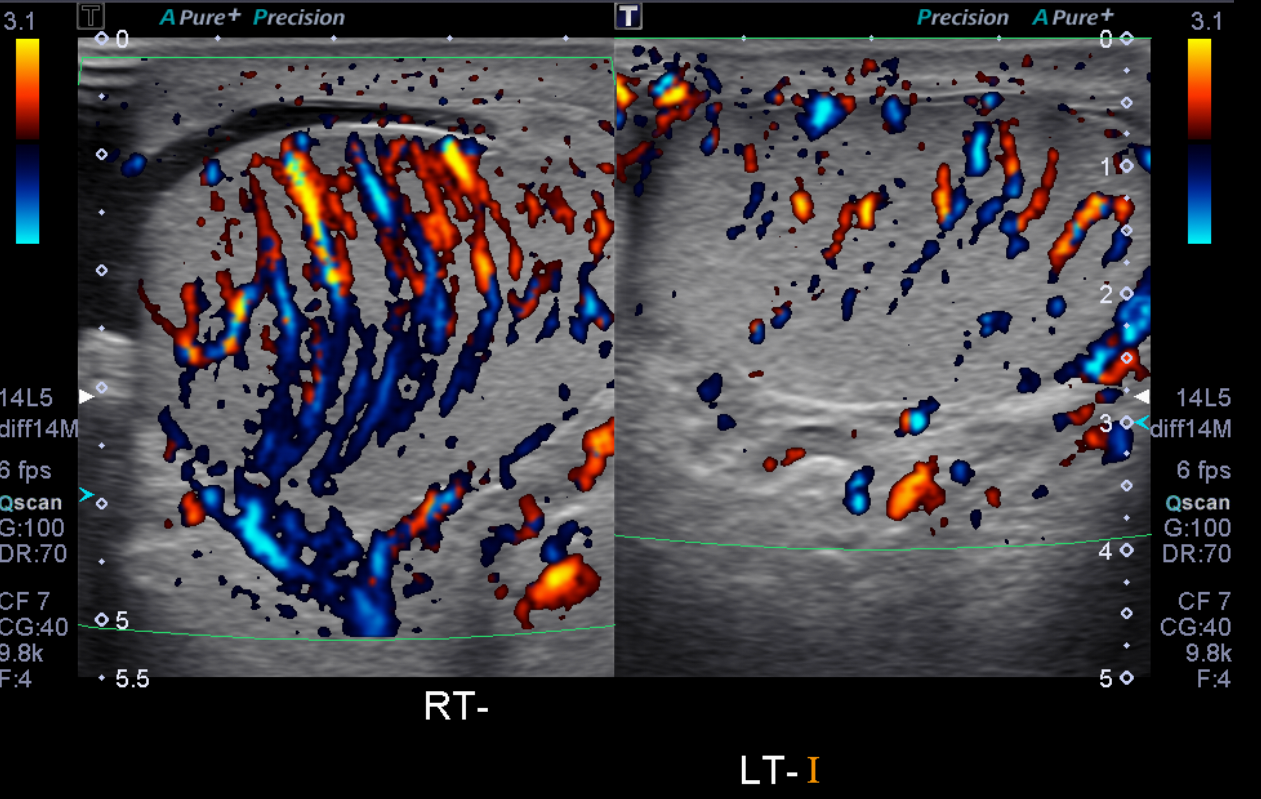
Scrotal Ultrasound
There is increased blood flow in which testis?
There is increased blood flow in the right testis on the color doppler images.
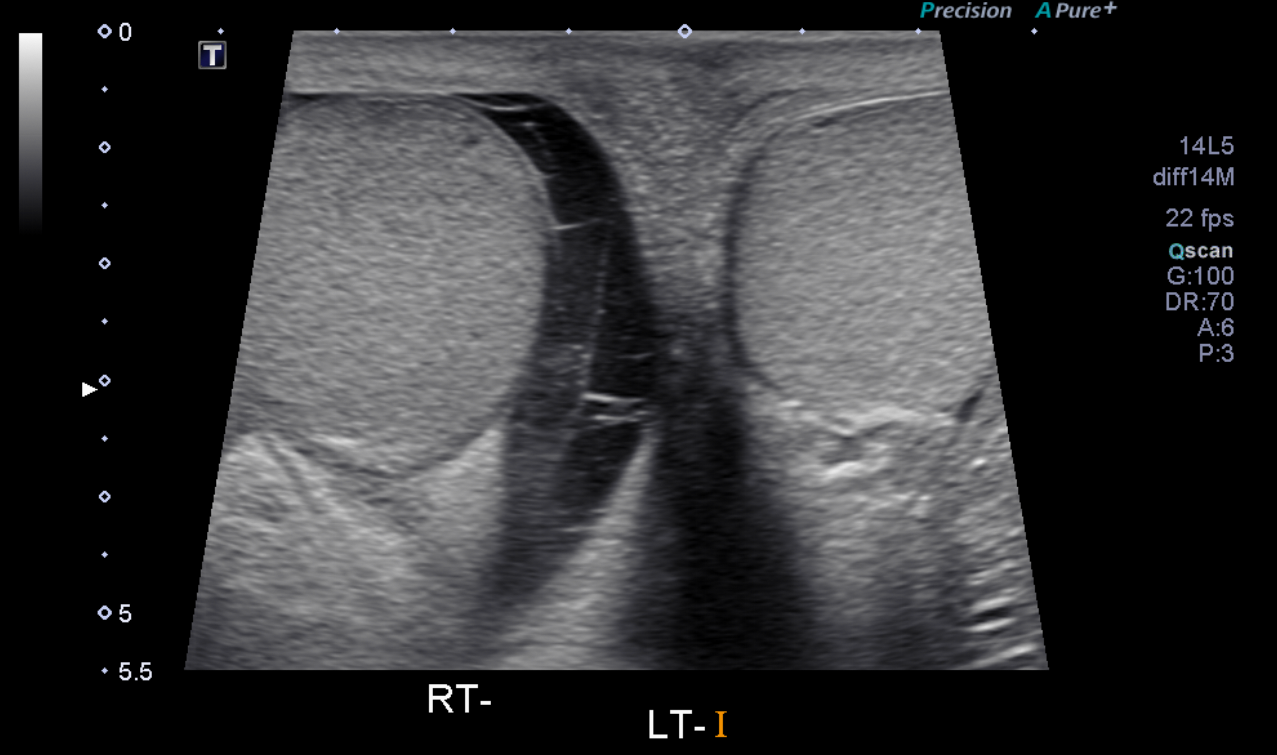
There is a fluid collection around which testis?
The hypoechoic (dark) region surrounding the right testicle is indicative of a fluid collection.
Is the fluid collection simple or complex?
This complex hydrocele contains septations, which make a pyocele or hematocele more likely.
View the full study if you'd like to take a look yourself.
Second Imaging Study
What is the next imaging study you will order?
No further imaging is needed.
Well done. You were correct
What is your Diagnosis now that you have seen the imaging results?
The patient’s clinical presentation and imaging findings are most consistent with epididymo-orchitis. Fournier’s gangrene is unlikely in this patient population, as it is a rare necrotizing soft tissue infection that is more common in older, diabetic, and immunocompromised patients. Testicular torsion is also less likely, as it typically presents with acute pain, a high-riding testis, and an absent cremasteric reflex.
Current Acuity
Initially, you selected and we suggested acuity.
Has your concern for this patient changed?
The patient requires routine, but expedited workup.
Assessment and Plan
Please provide your assessment and plan for this patient
The patient is a 25-year-old male with high-risk sexual behaviors presenting with right-sided scrotal pain, swelling, and erythema. Scrotal ultrasound findings are consistent with right epididymo-orchitis and a complex hydrocele. This patient should be started on antibiotics that cover sexually transmitted pathogens, most commonly gonorrhea and chlamydia. Pain management, scrotal elevation, and rest are also recommended. A follow-up with urology is needed to monitor response to treatment.
Lessons Learned:
- Differentiating epididymo-orchitis from testicular torsion is crucial as the latter is a urological emergency. Clinical signs such as relief of pain with testicular elevation (Prehn's sign) and a positive cremasteric reflex may suggest epididymo-orchitis over testicular torsion, but imaging is key to confirm the diagnosis.
- On ultrasound, epididymo-orchitis is characterized by an enlarged and hyperemic testis and epididymis, often with a reactive hydrocele.
- Further imaging or intervention may be required if a patient does not improve with treatment.
- Increased blood flow on doppler ultrasound is typically indicative of inflammation (as in epididymo-orchitis), while reduced blood flow is more indicative of testicular torsion.
- The most common causative organisms are N. Gonorrhoeae, C. Trachomatis and E. Coli.
Socioeconomic Factors: Risk factors for epididymo-orchitis include multiple sex partners, receptive anal intercourse, and lack of protection during intercourse, and poor hygiene.
That's the end of the module! Once you've reviewed the video(s), you can click here for another case challenge.
Next


{kind=link}
{kind=link}